MASCAL and CCP’s
Expect Heavy Losses
References: Ranger Handbook TC 3-21.76 | Infantry Rifle Platoon and Squad ATP 3-21.8

Overview
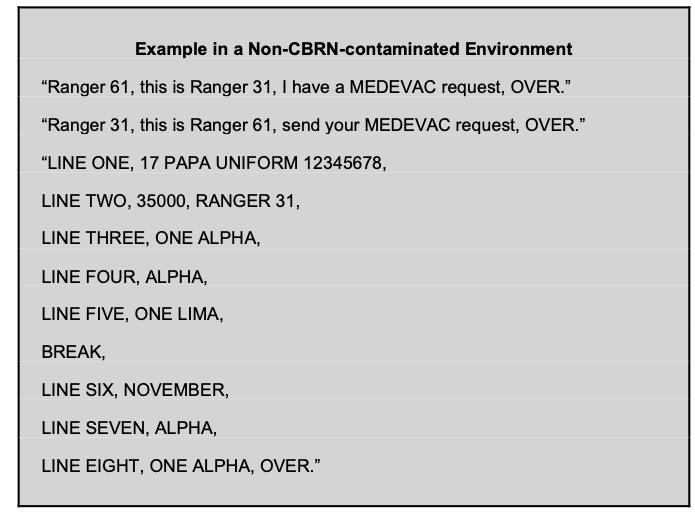
During your patrols, you will inevitably have multiple casualties. Because of this it is imperative that you have well marked CCP’s, HLZ’s and AXP’s You should also know how to use TCCC Cards and know how to call a 9 line MEDEVAC
Having a well prepared and rehearsed medical plan will give you a good score during Cadre evaluations especially if you are PSG
Key elements:
- Pre-planned Casualty Collection Points (CCPs), Helicopter Landing Zones (HLZs), and Ambulance Exchange Points (AXPs).
- Triage to prioritize care.
- Accurate TCCC cards for 9-Line MEDEVAC.
- Designated Aid & Litter teams.
CCP’s & Aid
During plan the PSG and Medic will create CCP, HLZ and AXP locations
- CCP: Concealed, defensible location near objective but outside enemy fire. Close to evacuation route.
- HLZ: Open area (minimum 35m diameter for UH-60) with no obstacles; mark with VS-17 panel or smoke.
- AXP: Roadside location for ground evacuation.
Be mindful of this when plotting your points The CCP should be close enough to provide immediate care but not so close where they can get fired at by the enemy. The best placement for a CCP is near an HLZ or AXP
About Rolling CCP’s
The term “Rolling CCP” Implies that the CCP will always be around 100 to 200 meters behind the assaulting element. This is acceptable during movement phases or an MTC, but when doing a fixed attack on a position, the CCP should be a marked location with coordinates
Added Tip: Plot multiple alternates; brief in OPORD Paragraph 4.
PSG Maintains the CCP He also assigns the medic and aid & litter team
After all patients are evaluated the PSG uses the TCCC cards to call in a 9 line, Refer to the MEDEVAC article for more info.
Establishing and Managing the CCP
After actions on objective:
- Medic/PSG designate CCP (concealed, covered).
- Aid & Litter teams move casualties to CCP.
- Medic conducts triage.
- Treat life-threatening injuries (MARCH).
- Fill TCCC cards.
- PSG consolidates cards; calls 9-Line MEDEVAC (see MEDEVAC article).
MASCAL & Triage
The best method to handle wounded in the CCP is to utalize the triage method
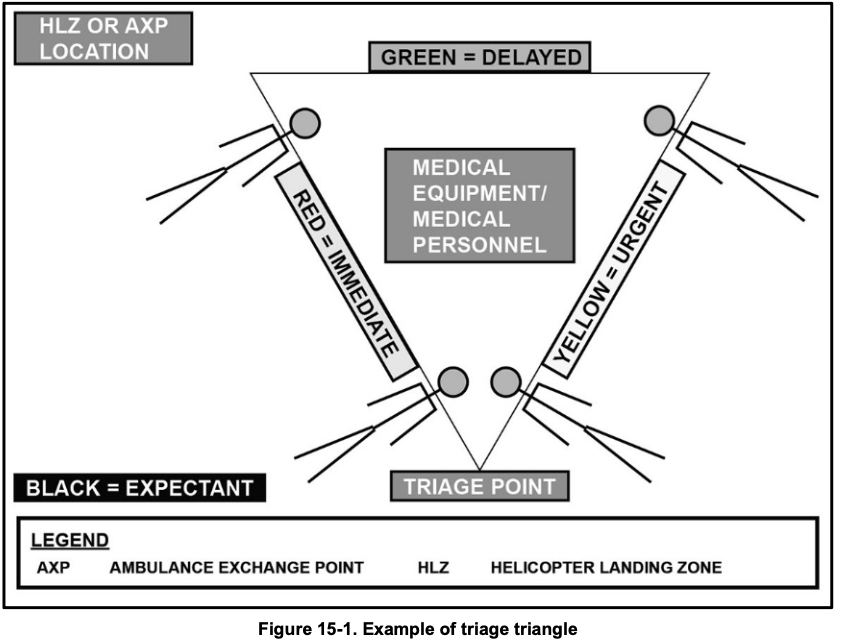
Use the triage triangle layout:
- Entry/exit at tip.
- Patients’ heads toward center.
- Segregate by category.
Triage Categories:
- Immediate: Requires urgent intervention to save life/limb/eyesight (e.g., massive hemorrhage, airway compromise).
- Delayed: Needs care but stable (e.g., penetrating wounds without arterial bleed).
- Minimal: Minor injuries; can return to duty (e.g., cuts, sprains).
- Expectant: Injuries incompatible with survival given resources (provide comfort; separate).
MASCAL means that you have more patients than the organic medial assets can handle most important actions in a MASCAL, are to triage patients appropriately, establish and manage the CCP leaders designate aid and litter teams before mission, maintain communication with higher
Actions to take include:
- Rapid triage.
- Maximize resources (use all IFAKs).
- Designate Aid & Litter teams pre-mission.
- Maintain security around CCP.
- Communicate status to higher.
Tips
- Rehearse casualty movement and 9-Line.
- Pre-designate teams in OPORD.
- Use all available personnel for litter carries.
- Mark CCP clearly (panel, chemlights).
- Practice TCCC under stress.
What not to do
- Delay triage — seconds matter.
- Treat in kill zone — move to cover first.
- Forget security at CCP.
- Mix categories — causes confusion.
- Call incomplete 9-Line.
Closing
Rehearsals are key in everything